CIDPUSA.org Autoimmune diseases
Electrical Stimulation Therapy
If 110 volts of electrical current is given to any human they will die instantly. A human can never become sensitized to electricity. Similarly a few milliamps of electricity will kill all Aids, Ebola, Dengue, TB or any other micro-organism. The bugs can never become resistant to electrical current.
D.C current is more deadly then AC. Only 50 volts of DC current can Kill a human , so a few milliamps of 9-15 volt DC current will kill all or any bug in the body in 15 minutes. If you repeat this application daily you will become resistant to any superbug in the world. All Russian astronauts use this device. To read how we have used this device please read the page and read the patients case reports.
CIDPUSA has tested this with a simple Tens unit and it works like magic. Allergies are gone, immune deficiency reverses, hair grow up , infertility is turned to fertility and infections are easily healed.One more interesting fact was that PTSD , drug addiction, sexual addiction was easily reversed at home with these units and they also helped in food poisoning, snake poisoning. If you used a unit you will not get food poisoning even though the food may be toxic enough to kill others.
. Years of vaginal infections easily reversed in 30 minutes of treatment with magnetic pulser, dermatomyositis reversed with a Tens unit and doxycycline, heart diseases and cancers disappear. All this from a simple tens unit.
Below is some history of electro treatment.

History and origin of electrostimulation, also commonly referred to as electrotherapy, is unique. The therapeutic benefits of electricity were not discovered in a laboratory or clinic and were not a byproduct of someone's accidentally coming into contact with a bolt of lightening. In fact, electrotherapy originates as early as 400 BC from contact with the torpedo fish, which could produce electric shocks between 100 and 150 volts. Taken live from lakes and streams and placed on a painful area of the body, the torpedo fish produced a series of electric shocks that reduced and controlled pain.
However, as with any new medical technology, electrotherapy was not readily accepted. This skepticism resulted in a decline of interest in electrotherapy toward the end of the [nineteenth] century (eMedicine Clinical Knowledge Base, 1996).
This therapeutic effectiveness in pain relief has led to other applications of electrotherapy by rehabilitative clinicians, including treating injured or diseased muscle and other soft-tissue conditions (Gersh, 1992).
This course reviews cell physiology and the response of muscle fibers to electrical stimulation, and presents the principles of electrical stimulation to aid the healthcare professional in decisions regarding indications and clinical applications.
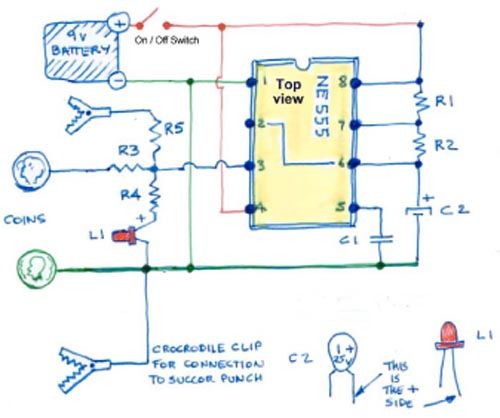
Below a circuit of a Hulda Clark zapper. Based upon the theory that 50 vols of DC will kill a human being then just a few milli amps of DC can kill any bug.
Services link
Zapper
Magnet therpay
Migraines magnetic
Magnetic treatment
Pulsed magnetic Rx
Magnetic stimulator
Antibodies in CFS
RTMS in depression
Magnetic stimulator
Niacin
Anti-ageing Magnets
RTMS in depression
Small Fiber neuropathy
Vinegar Benifits
Myositis
Healthy Oils
Vitamin-C
Home
Magnetic map
Treatment
Pathology
Women Disease
Fibromyalgia
IVIG
Diet anti-inflammatory
Burning Feet Home
Services Page
Autoimmune Ear
Autoimmune diseases
Sweet potatoes
Health Foods
Basil
ACV
Coconut oil Benefits