CIDPUSA.ORG Autoimmune Diseases
Brain Inflammation
ADEM:
Autoimmune diseases Guide CIDPUSA.ORG
Encephalitis
Encephalitis
What is Acute Disseminated Encephalomyelitis?
Acute disseminated encephalomyelitis (ADEM) is characterized by a brief but intense attack of inflammation in the brain and spinal cord that damages myelin the protective covering of nerve fibers.
ADEM
It often follows viral infection, or less often, vaccination for measles, mumps, or rubella.
The symptoms of ADEM come on quickly, beginning with encephalitis-like symptoms such as fever, fatigue, headache, nausea and vomiting, and in severe cases, seizures and coma.
It may also damage white matter (brain tissue that takes its name from the white color of myelin), leading to neurological symptoms such as visual loss (due to inflammation of the optic nerve) in one or both eyes, weakness even to the point of paralysis, and difficulty coordinating voluntary muscle movements (such as those used in walking). ADEM is sometimes misdiagnosed as a severe first attack of multiple sclerosis (MS), since some of the symptoms of the two disorders, particularly those caused by white matter injury, may be similar.
.
However, ADEM usually has symptoms of encephalitis (such as fever or coma), as well as symptoms of myelin damage (visual loss, paralysis), as opposed to MS, which doesn't have encephalitis symptoms. In addition, ADEM usually consists of a single episode or attack, while MS features many attacks over the course of time. Doctors will often use imaging techniques, such as MRI (magnetic resonance imaging), to search for old and new lesions (areas of damage) on the brain. Old inactive brain lesions on MRI suggest that the condition may be MS rather than ADEM, since MS often causes brain lesions before symptoms become obvious. In rare situations, brain biopsy may show findings that allow differentiation between ADEM and severe, acute forms of MS. Children are more likely than adults to have ADEM.
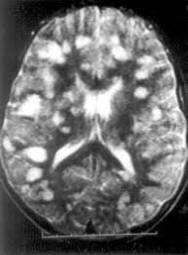 MRI
in A.D.E.M. showing white spots due to inflammation
MRI
in A.D.E.M. showing white spots due to inflammation
Is there any treatment?
Typical presentations of ADEM are with widespread neurological abnormalities, including multifocal signs in the brain, spinal cord, and optic nerves, and may include drowsiness or seizures. The classic pathological appearance is a perivenous lymphocytic inflammation with demyelinating lesions. The condition is usually precipitated by a viral infection or immunization (4). In the acute phase, MRI of the brain and spinal cord will show hyperintense lesions on T2-weighted and FLAIR images, although the underlying pathology may be oedema with minimal demyelination. Cerebrospinal fluid examination shows an increased protein level and leucocytosis, predominantly lymphocytes.
Our patient has strikingly classical MRI findings of ADEM in the brain. Together with clinical features of bilateral optic neuritis and the cerebrospinal fluid analysis results make the diagnosis of ADEM highly likely. One might argue that viral encephalitis should be considered as a possible alternative diagnosis given the CSF results. However the MRI findings are atypical. Multiple sclerosis and other demyelinating diseases were also less likely based on the patient's clinical, neuroimaging and CSF findings.
Although controlled studies are lacking, corticosteroids are the mainstay of treatment in ADEM. Plasmapheresis or immunoglobulins are an alternative if no satisfactory response is obtained (5). In a recent case report, early use of high dose corticosteroids was recommended for early recovery (6). Nishikawa et al (7) also reported successful treatment with IVIG, where three children ranging in age from 2 to 5 years with ADEM were successfully treated with high-dose IVIG. All patients were given IVIG at a dose of 400 mg/kg/ day for 5 consecutive days. The patients rapidly regained consciousness in 14 hours, 2 days, and 4 days and demonstrated complete clinical improvement within 18 days, 10 days, and 7 days of the initiation of the treatment, respectively.
What is the prognosis?
- Stiff person
- Takayasu
- Myasthenia General
- Study showing ALS
- A girl battles back from GBS
- A girl with stiff person syndrome
- Health benefits of ACV
- Low fat diet consequences
- Sunshine
- Chromium
- Acid Base
- Coffee Thyme
- Backpain antibiotics
- Autoimmune antibiotics
- Miracle cure ITP
- Pandas
- Terror Bug
- Electronic Frequency
- Candida
- Whipples
- Tetracycline
- Vitamins and cancer
- Cancer Regan
- MS & Virus
- Hair chemicals
- Osteoporosis
- See this message from God