NeuroMuscular Transmission disease
Myopathy Anterior Horn cell disease
😏cidpusa.org
3. Neuromuscular transmission defects
Only myasthenia gravis will be discussed further. This disease is characterized by abnormal fatigue with exercise. Myasthenia gravis commonly affects young woman and has a predilection for ocular, facial, masticator and proximal upper extremity muscles. Typically the patients recover to some degree after rest. Thus they feel much better in the morning, but become weaker as the day progresses. When the extraocular eye muscles are affected, diplopia (double vision) and ptosis (drooping of upper eyelid) are common and bothersome signs. This is an auto-immune disease with antibodies destroying the acetylcholine receptors (a postsynaptic defect).
Neuromuscular transmission defects
EMG findings:
Normal nerve conduction velocities, CMAP and SNAP amplitudes.
Decremental response on repetitive nerve stimulation.
Needle examination: Relatively normal MUPs.
Biochemistry:
Acetylcholine receptor antibodies are present in blood.
Histology:
Usually normal.
4. Primary muscle diseases (myopathies)
Muscle dystrophies (dystrophy = faulty development) are genetically determined diseases with onset at any time after birth. They are diagnosed on the pattern of muscle involvement. For example Duchenne muscle dystrophy is characterized by large calves, proximal muscle weakness and weakness of the latissimus dorsi muscles and pectoral muscles. Myotonic dystrophy patients show myotonia (an inability to relax a muscle after contraction) in addition to muscle weakness.
There also are congenital myopathies, metabolic myopathies and inflammatory myopathies that are beyond the scope of this course.
EMG findings:
Normal motor and sensory nerve conduction studies. The CMAPs are low
because of loss in muscle bulk. Needle examination show small MUPs.
Biochemical findings:
All progressive myopathies have increased CK blood levels indicating the
breakdown of muscle.
Histological findings:
Non-specific myopathic features such as large fibers, necrotic fibers, and
increased connective tissue.
b) Peripheral nerve diseases. Clinically characterized by the associated findings of sensory and autonomic abnormalities. EMG findings depend on whether it is primarily an axonal (axon cylinder) or demyelinating neuropathy; muscle histology shows type grouping and group atrophy with axonal damage; blood CK is normal.
c) Neuromuscular transmission defects. Clinically characterized by abnormal fatigability; EMG shows normal nerve conduction velocities, normal CMAP and SNAP amplitudes, decremental CMAP responses to repetitive nerve stimulation; muscle histology is relatively normal; blood CK is normal.
d) Primary muscle diseases. Clinically specific patterns of muscle weakness
may be noted; EMG shows normal nerve conduction velocities with low CMAP
amplitudes, normal SNAP amplitudes, needle examination shows smaller "myopathic"
MUPs; muscle histology shows myopathic changes; blood CK is elevated.
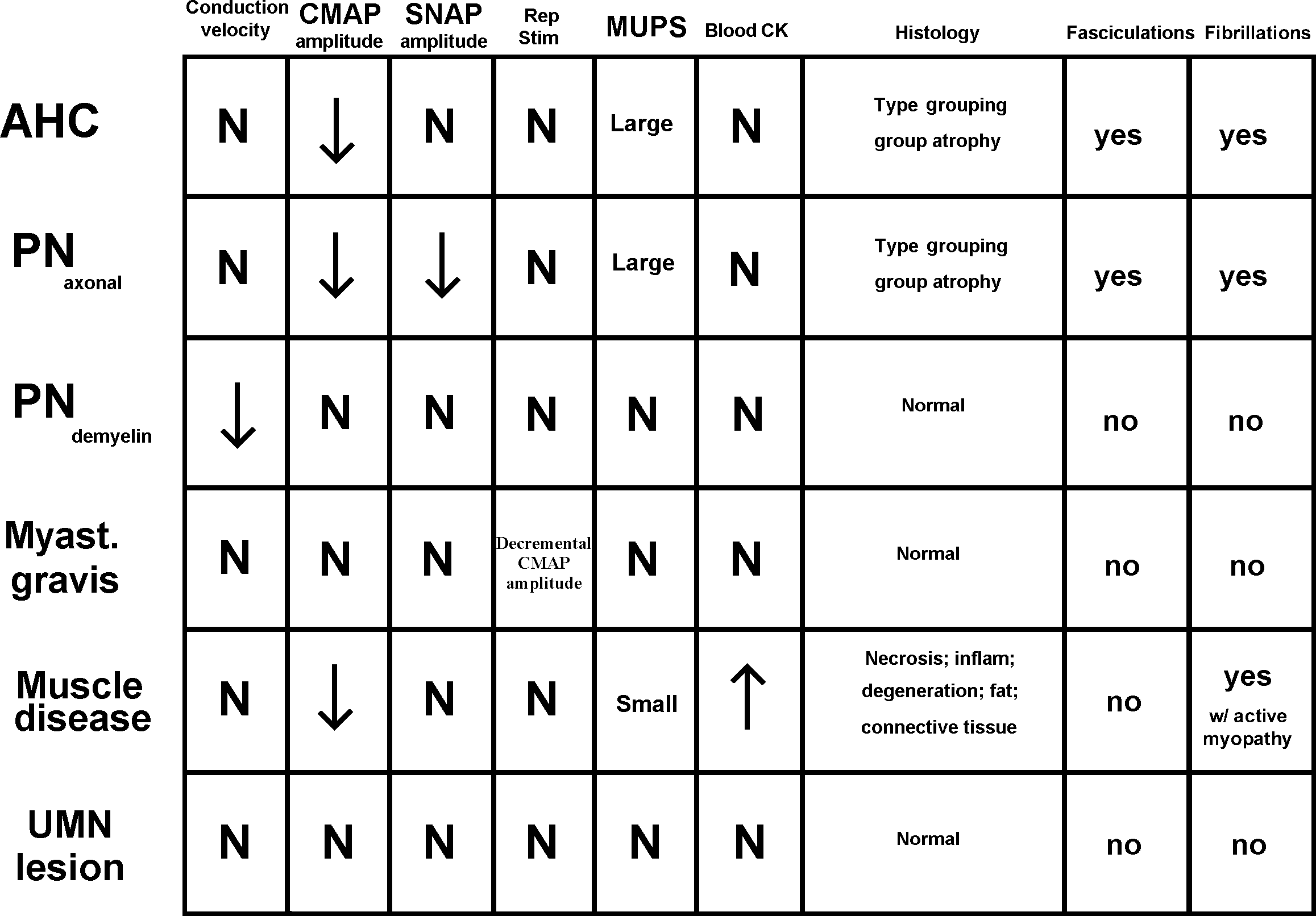 Figure 16
Figure 16continue to lower motor neurone next page
😏